The XDS-MS profile grew out of frustration trying to share summary information for a number of different kinds of care transitions. Dan began by classifying transfers of care into three types: Collaborative, Episodic (What I think of as Temporary), and Permanent. This picture comes from the IHE PCC Technical Framework Volume I and places the three types on two axes.
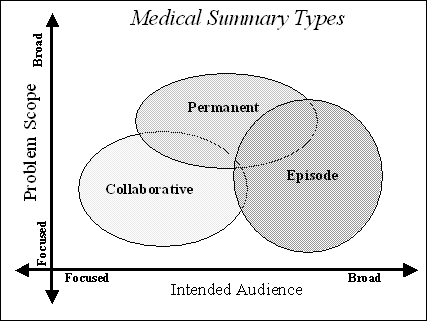
The two axes address whether the problems being addressed are broad (the whole patient) or focused on a specific topic (a condition or medical specialty), and whether the intended audience for the information is also focused (usually among the responsible care provider, the consulting physician and the patient), or which may involve several others, usually around a particular episode of care.
The Transfers of Care initiative is focused on the Collaborative and Episodic transfers (the "Green Button" proposed project was focused on Permanent Transfers). The easy way to think about Collaborative and Episodic transfers is to look at specific use cases for each.
Collaborative transfers most often occur during referrals to specialists for certain kinds of care. Another common case for collaborative transfer is dealing with perinatal care. In these cases, the patient's initial state of health is exchanged, along with some history about why the collaboration is needed. This often includes a narrative history of the present illness or condition (pregnancy is not an illness). During the collaboration, care provided by the specialist may necessitate changes in care given by other physicians engaged in patient care, especially when the collaboration is not short-term. Short-term collaborations fall into two main categories: Collaboration for diagnosis and collaboration for treatment. For diagnosis, the case is often pretty straightforward. An examination and some tests are performed, and the resulting diagnosis and recommended treatment(s) are communicated back to the referring provider, who then "takes back" responsibility for the patient's care, and initiates the recommendations in collaboration with the patient. For treatment, this can be short term, e.g., getting through a simple surgical procedure to correct the problem, again, after which the referring provider handles the follow-up and recovery. Longer term "collaborations" usually wind up affecting the patient in multiple ways and get broader in scope, so they usually would be classified as episodic.
Episodic transfers are most often exemplified by hospitalization or emergency care, after which the primary care physician handles follow-up and recovery. But not all episodic transfers are initiated by a hospitalization or emergency department visit. Some are long term activities that involve multiple parties. For example, treatment for cancer would be an episodic transfer, even if it involved no inpatient stay.
For the ToC project, I would recommend the following sets of use cases:
- Referral to a specialist for Diagnosis
- Referral to a specialist for Simple Treatment
- Referral to a specialist for Complex Treatment
- Heads up Referral to the ED
- Emergency Department Care requiring follow-up (with and without an accompanying inpatient stay)
- Hospitalization for an Episode of Care
For emergency care, again, they could use the HITSP C28 for the Emergency Department report and the C48 for the Discharge Summary. For the heads up referral to the ED, a slight variation on C48 exists in the IHE EDR profile, and I believe the necessary sections are already in C83.

0 comments:
Post a Comment